fear and anxiety
Fear: emotional response to a real or perceived imminent threat
- Surges of physical response: flight or fight
Anxiety: Anticipation of a future threat - Conceptually different
- Muscle tension and vigilance
- avoidance behaviors
Anxiety Disorders
- Most common mental health condition in the U.S.
- 22% women 14% men
- Differ in types of objects or sutiations that induce fear, anciety, or avoidance behavior, and the associated cognitive ideation
- Tend to be highly comorbid with one another
- CoMorbid
- denoting or relating to diseases or medical conditions that are simultaneously present in a patient.
- You can have more than 1 anxiety disorder
- Many develop in childhood and tend to persist if not treated
- Most occur more frequently in females than in males (approx. 2:1 ratio)
- Symptoms persist for 6 months or more, we start looking at it as more of a disorder, rather than phase in life
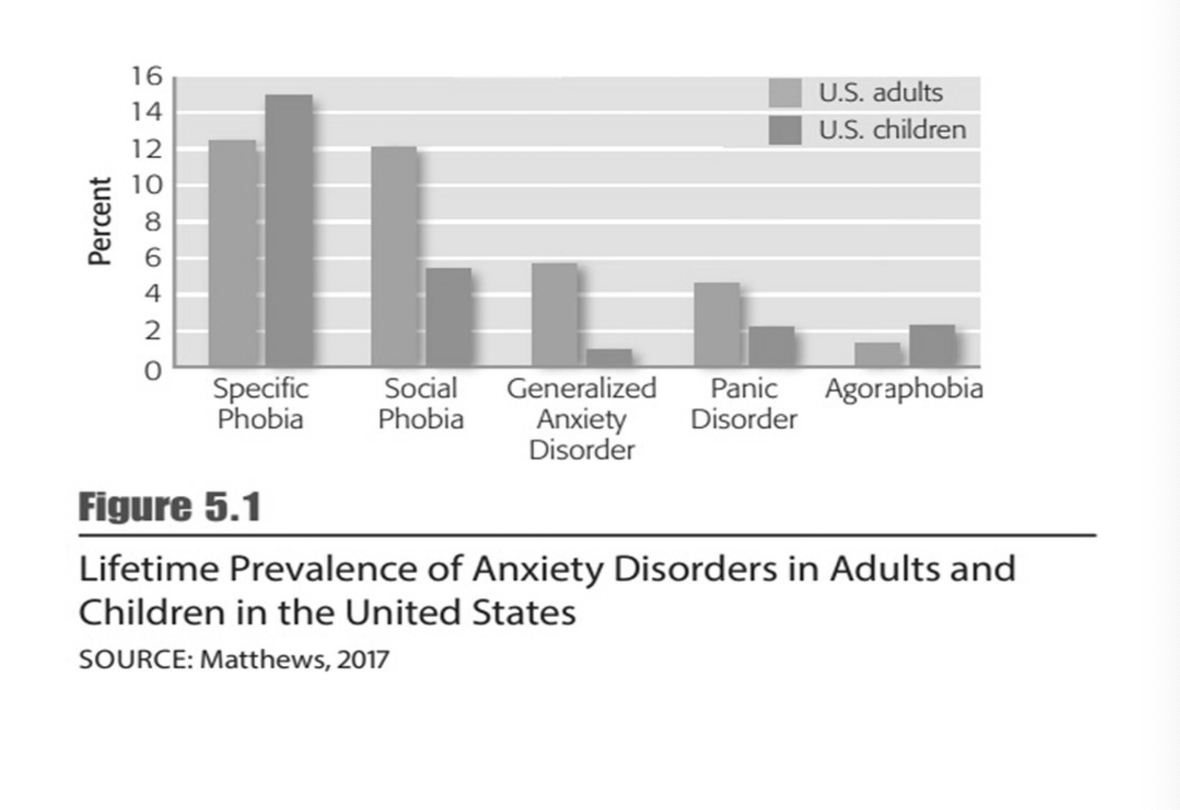
- Prevalence and Lifetime Morbidity Risk of Anxiety Disorders in the United States
- Ruling out medical or physical causes of anci4ty symptoms is important
- Medication side effects
- Excessive caffeine intake
- Hyperthyroidism
- Cardiac arrhythmias
- Withdrawal from alcohol
- Any substance use lmao
- People self medicate, which leads to more anxiety
Biological Dimension
Fear Circuitry in the Brain
- Centered in the amygdala, interacting with Prefrontal cortext and Hippocampus
Amygdala
Plays a central role in triggering state of fear or anxiety
- HPA activity triggers “fight-or-flight” response and in some cases a
“freeze” response - Primitive survival responses may take over and interfere with rational
thinking - starts the emotional ball rolling, what strats it
Sensory signals travel to hippocampus and prefrontal cortex
- Prefrontal cortex is slower, but is better at thinking things through
- Disables when in fear
- Process sensory input and evaluate danger
- Higher-level mental processing may result in signals to stop the HPA response
- Some studies have linked anxiety and fear with a reduction in GABA activity
- Neuroimaging techniques suggest that certain medications and certain therapies produce a reduction in limbic activity
- PET scans n stuff
- compares both anxiety people and non anxiety people, seeing how brains respond
- found overactivity in anxiety people
- Insufficent neurotransmitters
- Meds decrease oversensisitivty than therapy gets rid of thoughts
Genetic Influences
Serotonin
- Research focused on variation in serotonin transporter gene, 5-HTTLPR
- Result: short alleles of the 5-HTTLPR gene are associated with a reduction in serotonin activity and increased anxiety-related behaviors
- Anxiety can run in families
- Stressful environments help develop anxiety disorders
Numerous genes affect vulnerability
- Only influence an individual's predispositon
Psychological Dimension
- Psychological characteristics can interact with biological predispositions and produce anxiety symptoms
- Drinking way too much, then next day feeling anxious.
- Too much caffeine
- Anxiety sensitivity
- Common in those with disorders
- Negative appraisal
- Interpreting events as threatening
- Neutral situations can be interpreted negatively
- Skill of reappraisal
- Can evaluate other options, they can step back
- A sense of self-control and mastery also appears to reduce susceptibility to anxiety in humans
- Confidents that we can control ourselves and our actions can help reduce anxiety
Social and Sociocultural Dimensions
Daily environmental stress can produce anxiety
- People with biological or psychological vulnerabilities are most likely to be affected
- Predisposition and lack of psychological dimension skills
- Limited social support can cause anxiety
Factors
- Poverty, traumatic events, adverse working conditions, and limited social support
- Emergence of the COVID-19 illness significantly increased anxiety throughout the world
Gender plays a role in the development of anxiety disorders
- Women more frequently experience anxiety disorders compared to men
Culture can influence how anxiety is expressed
- Exposure to discrimination and prejudice can increase anxiety
- Internalized racism has been linked to increases in anxiety symptoms
- Acculturation conflicts also contribute to anxiety disorders
- In Western countries social anxiety involves fear of embarrassing oneself
- In some Asian countries social anxiety involves worries about being offensive to others
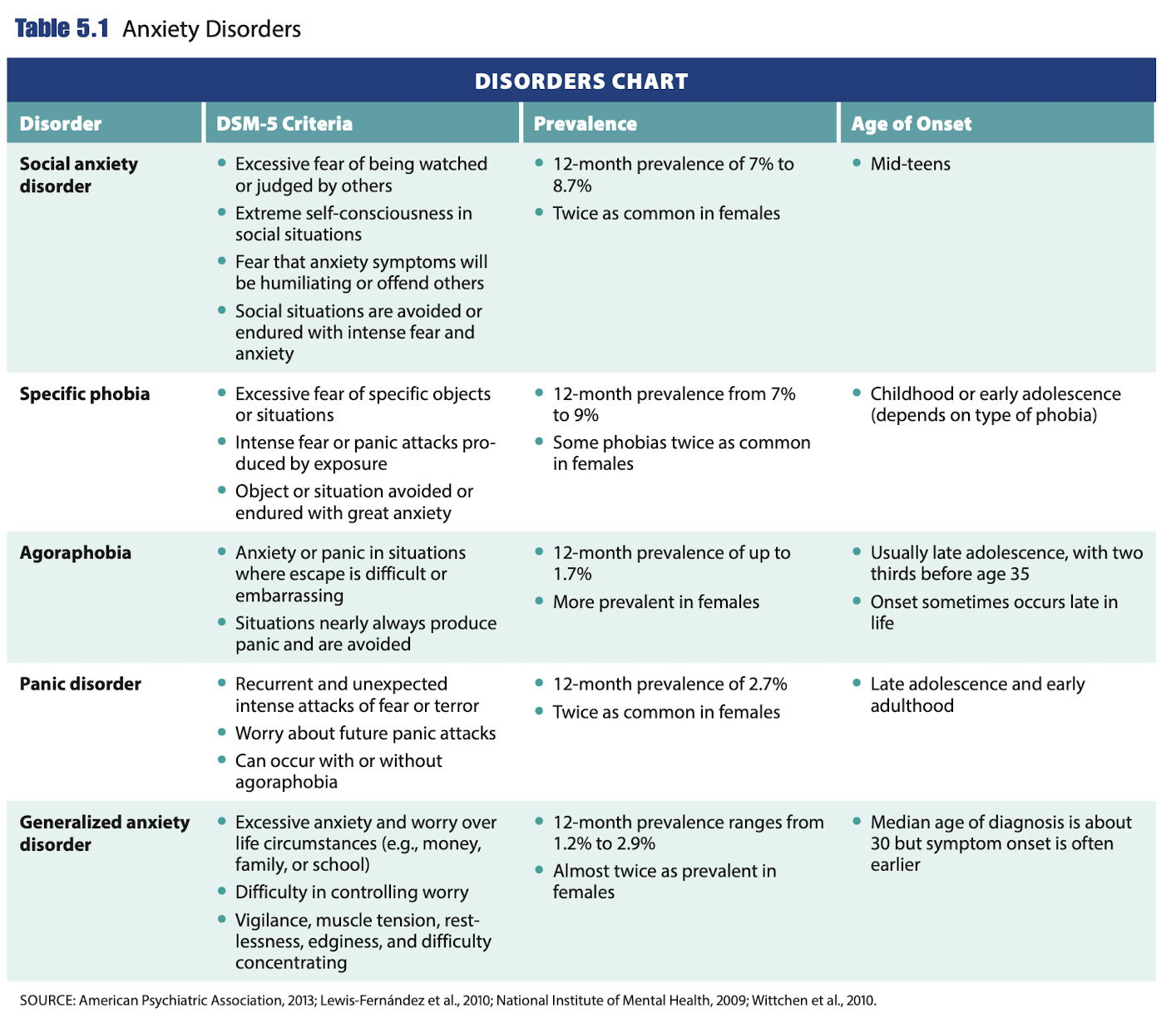
Phobias
Strong, persistent, unwarranted fear of a specific object or situation
- Extreme anxiety or panic is expressed when phobic stimulus is encountered
- Most adults recognize fear is excessive, but children may not
- Most common mental disorder in the United States
Categories of phobias
- social anxiety disorder
- specific phobias
- agoraphobia
Social Anxiety Disorder
- Intense fear of being scrutinized or doing something embarrassing or humiliating in the presence of others
- Women twice as likely as men to have social anxiety disorder
- Can be chronic and disabling
- Often comorbid with major depressive disorder, substance-use disorders, and suicidal thoughts or attempts
- Someone may be scared of eating infront of others
- This is the person who would drop out of school because they cannot do a presentation
- Very irrational thinking
- Cognitive process: being evaluated by others, judged
Specific Phobia
Extreme fear of a specific object or situation
- Exposure to stimulus nearly always produces intense anxiety or panic attack
- Immediate, dont need cognitive thought process
- Someone afraid of snakes doesnt think "im afraid of that snake" it is purely an irrational fear
- Common for one to have more than one specific phobia
- Average of 3 fears
- 75% have more than one phobia
Primary Types
- Living creatures (example: spiders)
- Environmental conditions (example: heights)
- Blood/injection or injury (example: needles)
- Situational factors (example: flying)
Agoraphobia
- Intense fear of at least two of the following:
- Being outside of the home alone
- Traveling via public transportation
- Being in open spaces
- Being in stores or theatres
- Standing in line or being in a crowd
- Situations are feared because escape or help may not be readily available
- In some cases, people refuse to leave their homes due to concern they might have a panic attack
- Older adults might fall
- Always cause panic, so they avoid or go with companion
Social Dimension
- Parental behaviors influence development of social anxiety in children
- Over protection
- Lack of support for independence/ learning how to be independent
- Negative family interaction patterns and family stress
- Associated with social anxiety in middle childhood
- Punitive maternal parenting style
- Victimization by peers during childhood
- Ongoing ostracism and bullying maintain and exacerbate social anxiety symptoms
- Kids can have intense fear of going to school
Sociocultural Dimension
- Women and girls are more likely to have phobias
- Some objects of phobia trigger both fear and disgust responses
- Disgust response stronger in females
- Gender differences may be due to a combination of biological and temperamental factors
- Social norms and socialization experiences
- There are fewer gender differences for ear of bodily injury and enclosed spaces
- Sad is more common in collectivistic cultures
- Individual behaviors seen to reflect on entire family or group
- Use of shame as a method of parental control
- Discrepancies between traditional cultural behavioral norms and mainstream culture
- Other Cultural Factors
- A strong sense of personal responsibility for social behaviors
- A perceived need to follow a set of rigid moral codes and rituals
- The threat of being ostracized for deviations from social norms
- Prejudice and discrimination from the mainstream culture
Biological Treatment of Phobias
Medications with efficacy for SAD
- SSRI (antidepressants)
- Often prescribed for chronic forms of anxiety
- SNRIs and MAOIs
- Beta-blockers
- Benzodiazepines increase GABA activity
- Examples: Ativan, Xanax, Valium
- Can produce dependence
- Cognitive deterioration or fall-related injury in older adults
- Examples: Ativan, Xanax, Valium
Cognitive-Behavioral Treatments
- Exposure Therapy
- Systematic desensitization
- Imagine situation
- Flooding
- Repeatedly placed in feared situation
- No relaxation
- Gradual buildup or just thrown in the depend
- Modeling
- Individual watches another confront object or situation
- Gradual introduction to the feared situation
- Applied tension
- Smartphone apps and virtual reality therapy
- Systematic desensitization
- Cognitive Restructuring
- Identifying and changing irrational thoughts
- Therapist challenges false thoughts, "Is that really whats happeing?"
- Systematic desensitization
- Exposure techniques with relaxation
- Modeling therapy
- Viewing another person’s successful interactions with the subject of the phobia
Panic Disorder
Panic Attacks
- Prominent feature of anxiety disorders as type of fear response, but is also in other mental disorders
- Quick, Immiediate, physical, reaches peak fast
- Can be expected
- Recurrent, unexpected panic attacks
- Combined with apprehension about having another attack or behavior changes designed to avoid having another
- Reactions present for 1 month or more to be considered disorder
- Most diagnosed with Panic Disorder also have Agoraphobia
- Cultural variations in how symptoms are expressed
- Caucasians generally report cardiac and respiratory symptoms
- Cambodian refugees may have somatic symptoms
- African Americans may experience numbing sensations in their extremities and fears of dying
- Indigenous/American Indians may report a pounding heart, dizziness, and altered perceptions of time
- Past-year prevalence rate in the United States is 2.7 percent
- Twice as common in women as in men
Psychological Dimension
- Individuals show heightened fear responses to bodily sensations
- Cognitive-Behavorial perspective
- Unpleasant bodily sensations are misinterpreted
- Inaccurate cognitions and symptoms create a feedback loop that increases anxiety
- A decrease in panic-related cognitions and anxiety sensitivity is associated with a subsequent reduction in panic symptoms
Role of Cognitions in Panic Attacks
Biological Treatment of Panic Disorders
SSRI Antidepressants
Tricyclic antidepressants
Benzodiazepines (risk of dependency)
- 45% of people dont respond to medication
Cognitive-Behavioral Treatment of Panic Disorder
- Educating the client about panic disorder
- Identifying and correcting catastrophic thinking
- Teaching client to self-induce physiological symptoms in order to extinguish the conditioning
- Encouraging client to face the symptoms
- Reviewing the skills acquired and making a plan to prevent relapse
Generalized Anxiety Disorder (GAD)
Persistent, high levels of anxiety and excessive, difficult-to-control worry over life circumstances
- Work, school, interpersonal relaitonships
- Sooo difficuilt to stop worrying
- DSM-5 diagnostic criteria
- Symptoms must be present on the majority of days for 6 months
- Causes significant impairment in life activities
- About 2.7 percent of the U.S. adult population is affected
- Lifetime prevalence among adolescents is 2.2 percent
- Women and girls are nearly twice as likely to receive this diagnosis compared to men and boys
Treatment of GAD
- Drug Therapy
- Benzodiazepines—Issues with dependence
- Antidepressants—Lower less risk of dependence
- Cognitive-behavorial therapy
- Effective psychological treatment
- Mindfulness practice
- very important, teach relax
Obsessive-Compulsive and Related Disorders
- More common in boys as children
- More common in women and girls in adolescents and adulthood
Obsession: - consistent, anxiety producing thoughts or images
Compulsion: - overwhelming need to engage in activities or mental acts to counteract anxiety or prevent occurrence of dreaded event
- In response to obsession
Hoarding Disorder
- Inability to discard items regardless of their value
- Perceived need for items and distress over the thought of giving or throwing them away
- An accumulation of items that produces congestion and clutter
- More common among women and in older adults
Other Types of OCD-Related Disorders
Body dysmorphic disorder
- Preoccupation with a perceived physical defect, repetitive behaviors, and distress or impairment in life activities
- Up to 60 percent of individuals with BDD undergo unnecessary cosmetic surgeries
- Muscle dysmorphia
Trichotillomania - Hair ripping
- Despite trying to stop, pull and rub their hair
Excoriation - mental health condition where you compulsively pick at your skin
OCD vs TIC Disorder
Compulsion = ritualized, overt, or covert behaviors
OCD = Compulsions (thoughts or actions) may be performed to neutralize obsessions or reduce distress/anxiety
Tic = sudden, repetitive, stereotyped motor movements or phonic productions that are often perceived as involuntary but that are sometimes accompanied by premonitory sensory urges
- occur in bouts, vary in intensity, and wax and wane in severity
Suicidal Obsession
Suicidal ideation = range of contemplations, wishes, and preoccupations with death and suicide
- Other things along with this, lke depressive and sad mood
Suicidal Obsession (Self-Harm OCD) = intrusive thoughts about losing control and committing suicide - Part of OCD, persons thoughts are incongruent with mood. (Dont want to kill self but think bout it)
Etiology of Obsessive-Compulsive and Related Disorders
- Heredity is involved
- Non-shared environmental influences are equally important
- Endophenotype (bio or psych phenomenon of disorder) characteristics for OCD
- Impairment in:
- Decision making, planning, and mental flexibility
- Associated with less volume in certain regions of the prefrontal cortex (Parietal lobe)
- Dysregulation of the orbitofrontal-caudate circuit (orbitofrontal-striatal circuit)
- Impairment in:
Psychological Dimension of OCD
- Behavioral Perspective
- Obsessive-compulsive behaviors develop because they reduce anxiety
- Cognitive Characteristics
- Exaggerated estimates of probability of harm
- Control
- Intolerance of uncertainty
- Thought fusion
- Disconfirmatory bias
- thinking about bad act is just as bad as doing it
Social and Sociocultural Dimensions
Family variables
- Controlling, overly critical parenting styles
- Low parental warmth
- Discouragement of autonomy
- Overprotective parents with rigid rules
- Perceiving relatives to be critical or hostile can increase symptom severity
- On rare occasions, living with a partner or family member with OCD can produce a shared psychopathology
Treatment of Obsessive-Compulsive and Related Disorders
Biological Treatments
- SSRI
- Deep Brain Stimulation
Behavorial Treatments
- Exposure therapy
- Gradual exposure or flooding
- Response preventiony